

Abstract
Background: Incidence of diffuse large B cell lymphoma (DLBCL), an aggressive but curable Non-Hodgkin Lymphoma (NHL) is increasing in the oldest old. Treatment of these patients is challenging due to advanced age, concomitant comorbidities present in this population and the paucity of data from this population in clinical trials.
Aims: to evaluate which parameters are considered by medical oncologists in the management and systemic treatment of DLBCL in the oldest old patients (³80 years old) in our centers.
Method: This retrospective study evaluated the management of 118 patients ³80 years old diagnosed with DLBCL between 2006 and 2016 in two Quebec hospitals. Baseline demographics, systemic chemotherapy regimens, and overall survival were obtained. Documentation of patient characteristics influencing management options offered by medical oncologists was analyzed when available.
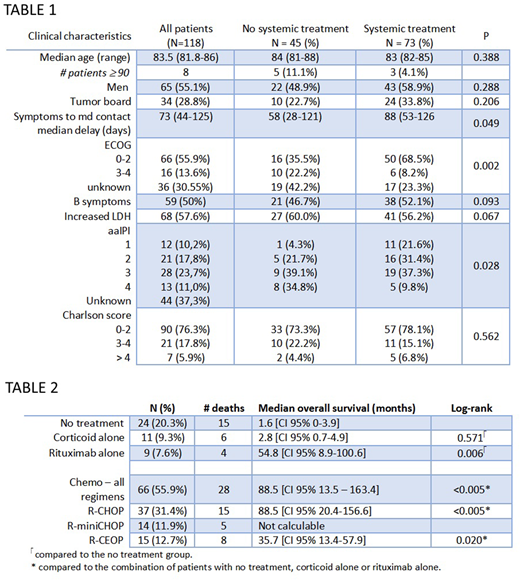
Results: Median age was 83.5 years, maximum age was 96 years old, with a total of 8 patients aged ³90 years, and included 65 (55.1%) men. Median Charlson score was 1 [0-2], with 28 (23.7%) patients having a Charlson score > 2. Main patient characteristics according to management are reported in table 1.
Of all 73 patients who received systemic chemotherapy, 38 (52.1%) had either a complete or partial response. Median overall survival (OS) of patients treated with systemic chemotherapy (either rituximab alone, R-CHOP, R-mini-CHOP or R-CEOP) was 54.8 months [95% IC 15.7-93.9 months] compared to 4.6 months for patients that did not received systemic chemotherapy [95% IC 0-12.6 months], p < 0.005. Median number of chemotherapy cycles was 3 (1-6), with 19 patients whom received 6 to 8 cycles. 33 (28%) of the cohort received radiotherapy, mostly as an adjunct to the systemic treatment: only 5 patients received radiotherapy alone. Median OS for the different chemotherapy regimens are reported in table 2.
54.8% of the treated patients received prophylactic G-CSF. Febrile neutropenia developed in 13 (17.8%) patients, 10 of whom were prophylactically treated with G-CSF. We observed 54 deaths in our cohort. Main cause of death was lymphoma: 12 in the untreated group (N= 44) and 7 in the treated group (N= 73). Other known causes were sepsis, heart failure, and respiratory failure.
Comorbidities were mentioned as influencing treatment option in 33 files: 16 did not receive systemic treatment whereas 17 received systemic treatment. Median Charlson score for these patients was 2 [1-3]. 14 patients had documented geriatric syndromes (i.e. dementia, malnutrition, frailty, delirium or functional decline) as the main concern for treatment; 9 of them did not receive systemic chemotherapy.
Conclusion: Very elderly DLBCL patients, despite their advanced age, still have a significant survival benefit when treated with systemic chemotherapy. In our study, main factors contributing to overall survival were ECOG status and aaIPI as they are known to be important considerations in the management decision process. Interestingly, comorbidities, as measured by the Charlson score, do not seem as important in the management decision process. Instead, geriatric syndromes, some of them potentially reversible, appear to play an important role.
Pavic:Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; BMS: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Novartis: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; AstraZeneca: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Roche: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Takeda: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal